| Origin | Transverse processes of vertebrae C1, C2, C3 and C4 |
| Insertion | Superior part of the medial border of the scapula |
| Action | Elevates the scapula Tilts the glenoid cavity inferiorly by downwardly rotating the scapula Neck extension and lateral flexion |
| Nerve | Dorsal scapular nerve (C4, C5) Cervical nerves (C3, C4) |
| Artery | Dorsal scapular artery |
Location & Overview
The levator scapulae muscle is situated on the upper back and lateral side of the neck, extending from the cervical spine to the shoulder blade. The inferior part of the muscle is covered by the trapezius muscle, a large superficial muscle that spans the neck, shoulders, and back. The superior part of the levator scapulae is covered by the sternocleidomastoid muscle, a prominent superficial muscle of the neck [1]. Additionally, the levator scapulae is located in the middle of the posterior triangle (or lateral cervical region) of the neck. The posterior triangle of the neck has three borders, the sternocleidomastoid anteriorly, the trapezius muscle posteriorly, and the middle 1/3 of the clavicle inferiorly [2] [3]. The levator scapulae muscle, as the name implies, primarily functions to elevate the scapula, an action signified with its Latin etymology – ‘levare’ meaning ‘to raise’.
The levator scapulae can be involved in numerous pathologies. For example, snapping scapula syndrome, also known as scapulothoracic bursitis, often involves the levator scapulae [4]. This condition presents with a grating, snapping, or popping sensation in the shoulder blade, often resulting from bony abnormalities, overuse injuries, or muscle imbalances around the scapula, including the levator scapulae.
Levator scapulae syndrome is another condition [5], which is characterised by pain and stiffness in the neck and shoulders, specifically at the points of the levator scapulae’s attachments. This condition typically arises from poor posture or chronic muscular stress, which leads to muscle overuse and strain.
Another pathology is prengel deformity [6], a congenital condition which results in an abnormally high positioning of the scapula. This condition often involves abnormal development or functioning of the levator scapulae. This can impact shoulder movement and may require surgical correction.
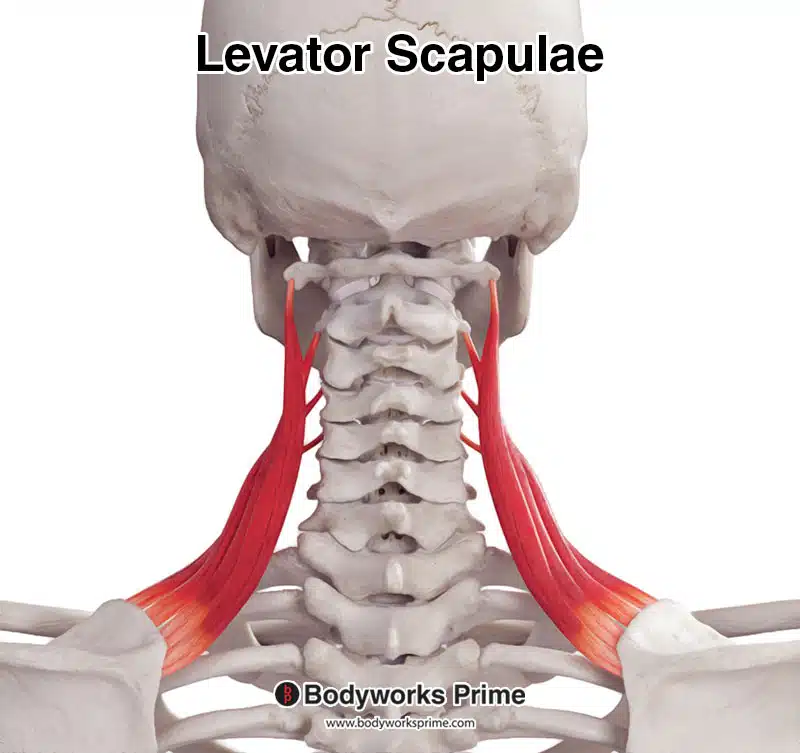
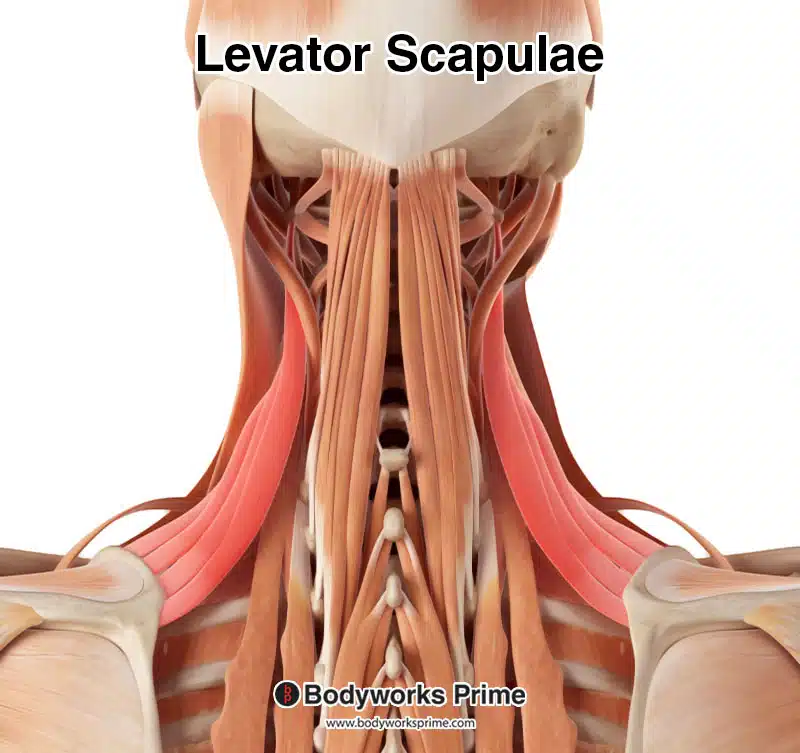
Here we can see the levator scapulae from a posterior view.
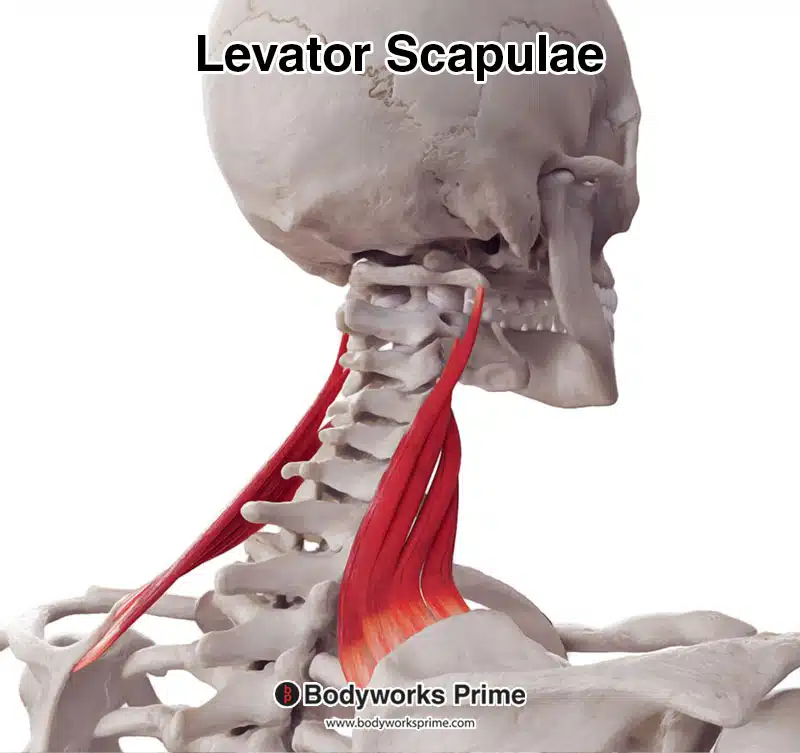
Here we can see the levator scapulae from a posterolateral view.
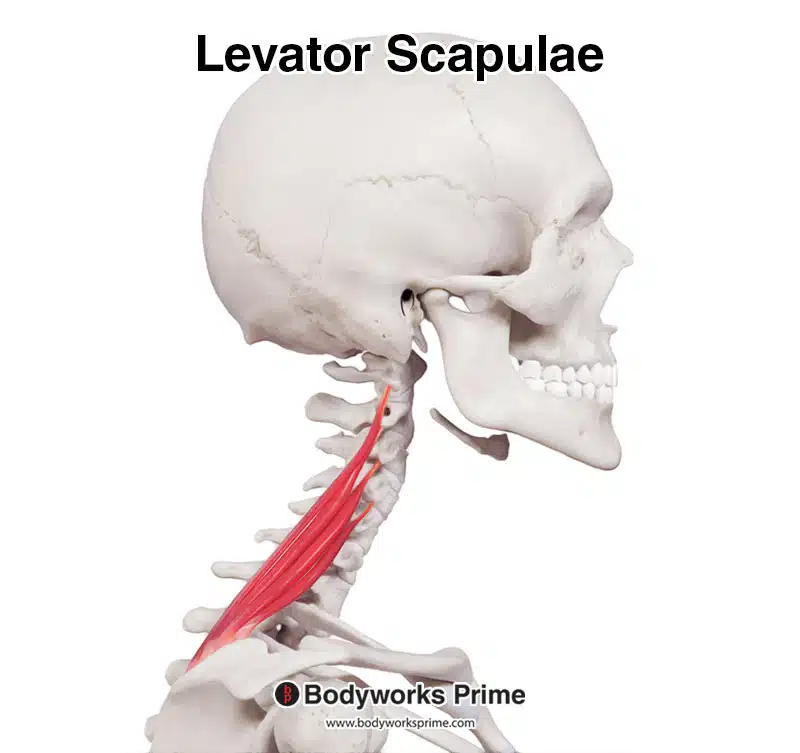
Here we can see the levator scapulae from a lateral view.
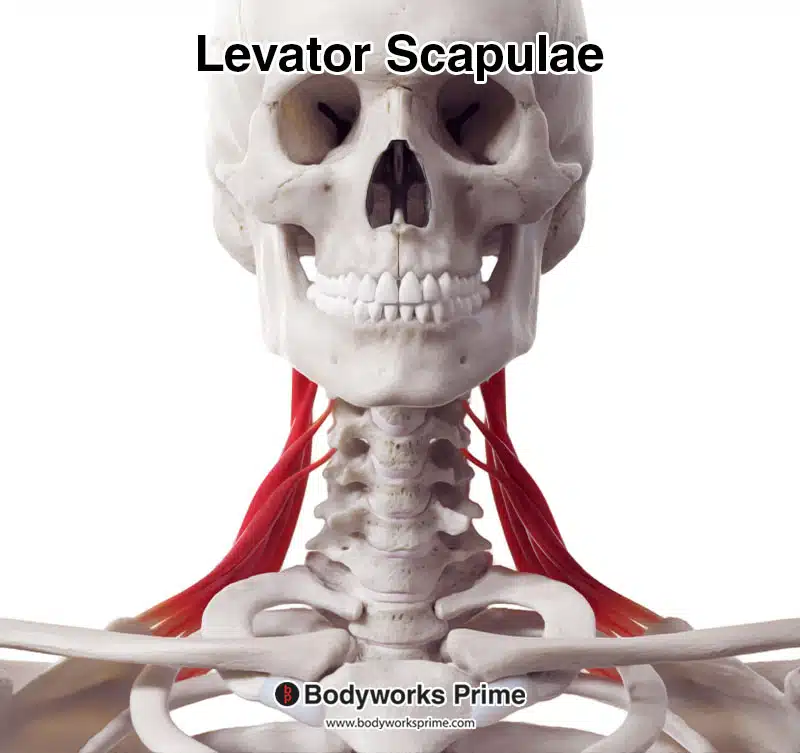
Here we can see the levator scapulae from an anterior view.
Here we can see the levator scapulae highlighted in red amongst the other muscles of the body, seen from a posterior view. Muscles which are superficial to the levator scapulae have been removed to reveal its location.
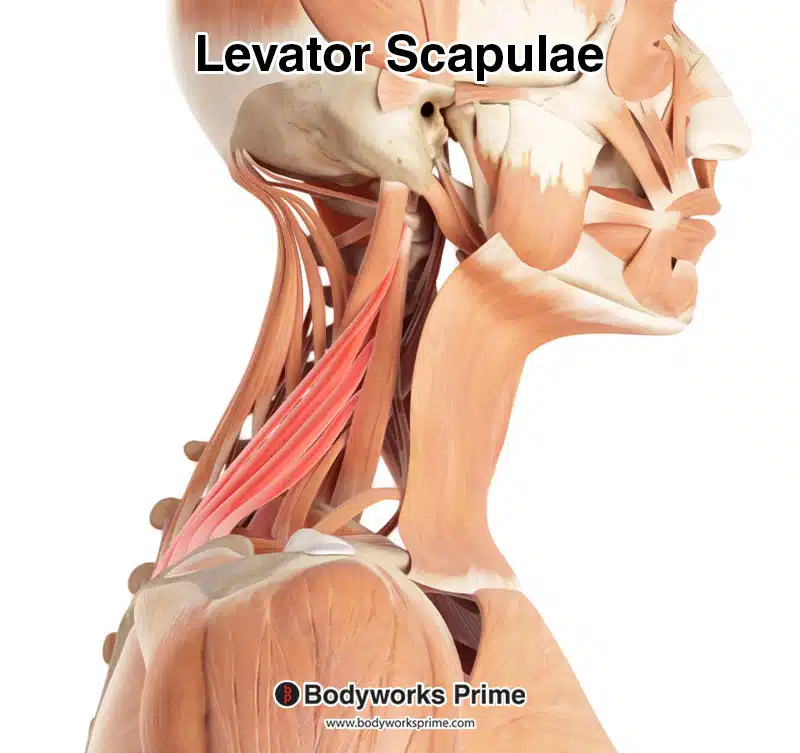
Here we can see the levator scapulae highlighted in red amongst the other muscles of the body, seen from a lateral view. Muscles which are superficial to the levator scapulae have been removed to reveal its location.
Origin & Insertion
The levator scapulae muscle originates on multiple points along the cervical vertebrae. The levator scapulae muscle originates from the posterior tubercles of the transverse processes of vertebrae C1, C2, C3 and C4 [7] [8] [9] [10]. These cervical vertebrae are found in the neck region. The atlas is the first vertebra and it supports the skull. The axis is the second vertebrae down that allows rotation of the head. C3 and C4 are located directly below the axis. The transverse processes in the cervical region each have an anterior and a posterior tubercle. The posterior tubercle serves as the point of attachment for muscles, including the levator scapulae. The posterior tubercle is a small, rounded bony prominence located on the back part of each transverse process [11] [12].
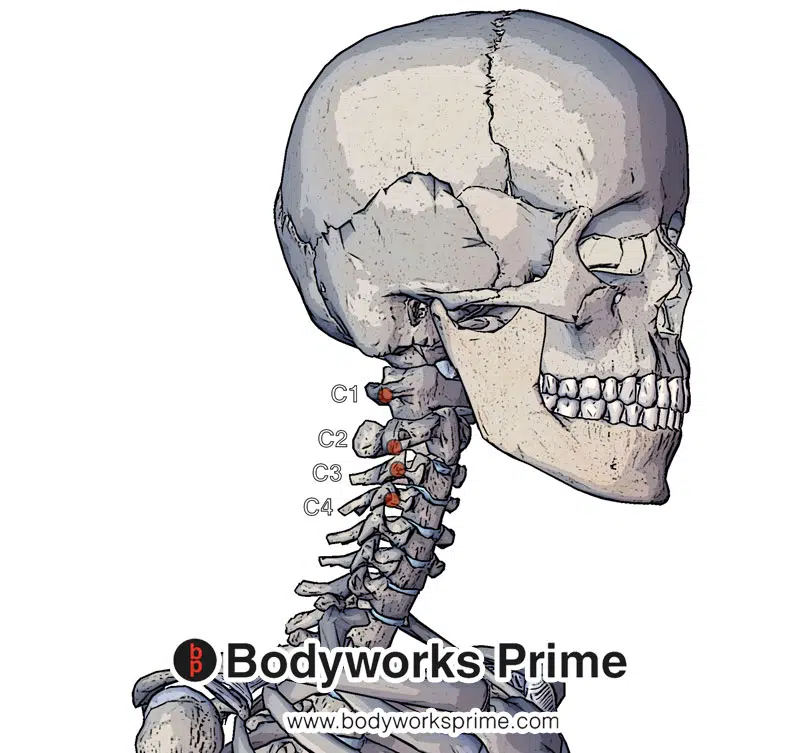
Pictured here we can see the origin of the levator scapulae muscle. The levator scapulae originates from the posterior tubercles of transverse processes of C1 to C4 vertebrae.
The muscle fibers of the levator scapulae course downwards and laterally from its origin, towards the scapula. They then insert on the posterior part of the medial border of the scapula, between the superior angle and the root of the scapular spine [13] [14] [15] [16]. The scapula, also known as the shoulder blade, is a triangular bone located on the upper part of the back. The superior angle refers to the uppermost point of the scapula, where the medial and superior borders meet. The root of the scapula’s spine is located on the medial border of the scapula, where the spine of the scapula begins [17] [18].
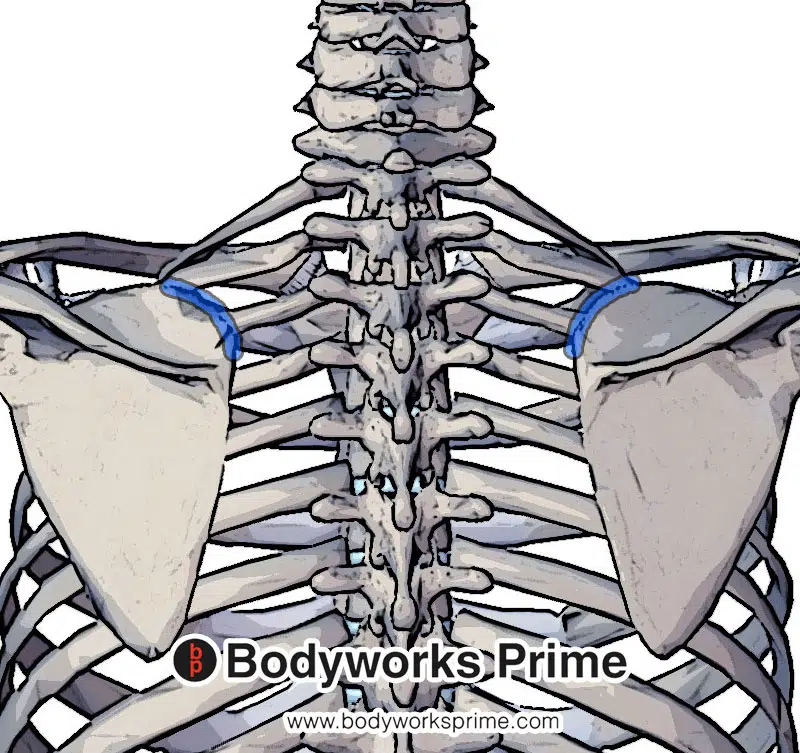
Pictured here we can see the insertion of the levator scapulae muscle. The levator scapulae inserts at the superior part of the medial border of scapula.
Actions
The primary actions of the levator scapulae involve movements of the scapula and the neck because the muscle exerts its pull between these two regions. The most notable action of the levator scapulae, as suggested by its name, is the elevation of the scapula [19] [20]. This action can be visualised when shrugging the shoulders, where the scapulae are drawn upward towards the head.
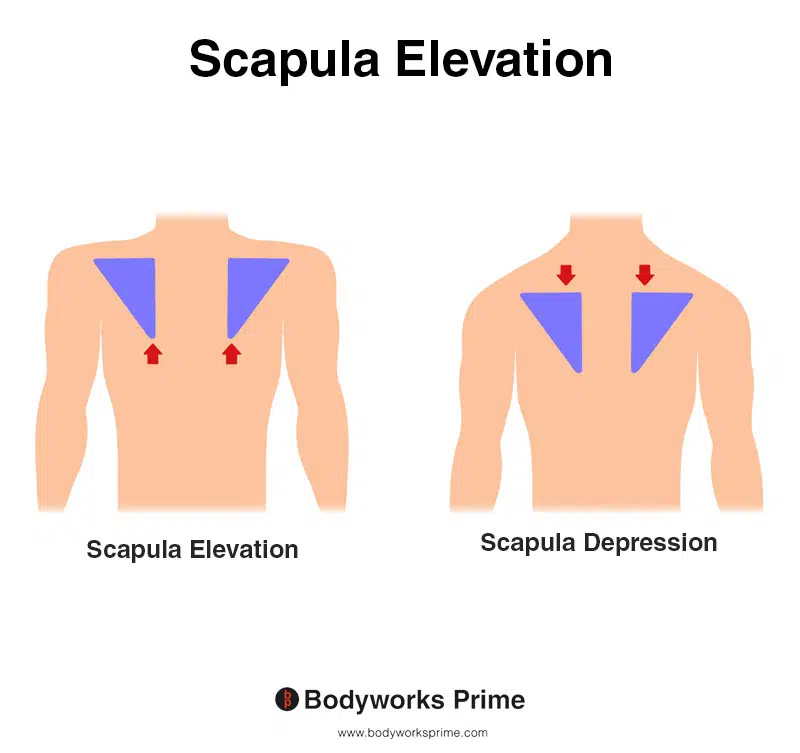
This image shows scapula elevation, where the shoulder blade moves upward, drawing the shoulder joint superiorly. This movement happens when shrugging the shoulders upwards. The opposite of scapula elevation is scapula depression. The levator scapulae can elevate the scapula.
In addition to elevation of the scapula, the levator scapulae also contributes to the downward rotation of the scapula. It works alongside the following muscles to accomplish this: the rhomboids, descending fibers of the trapezius, latissimus dorsi, pectoralis major and pectoralis minor [21] [22]. Downward rotation of the scapula involves turning the scapula so that the glenoid cavity, where the humerus articulates, moves downward. This movement can be seen when the arm is moved from a raised position back to the side of the body.
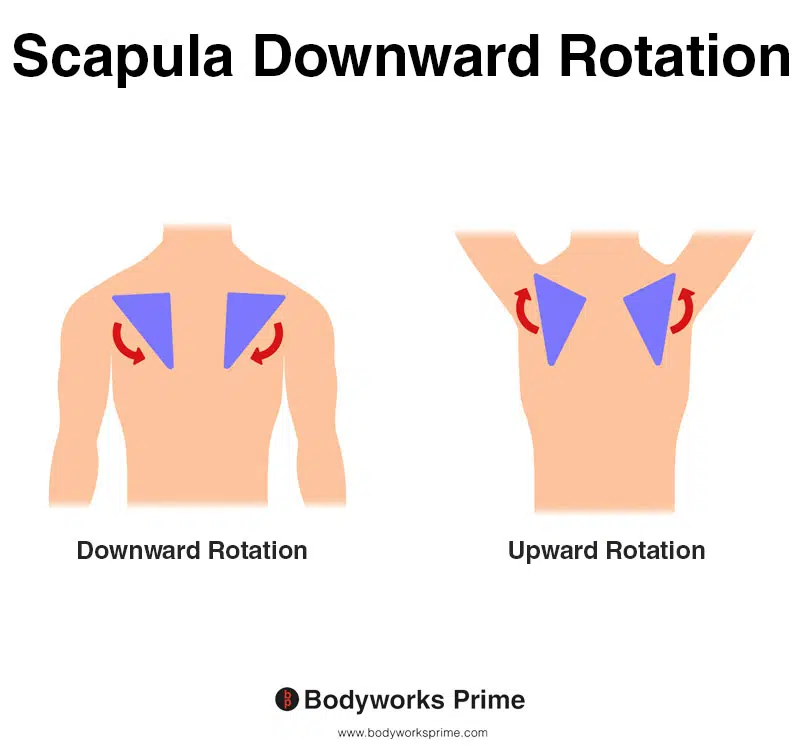
This image shows scapula downward rotation, where the shoulder blade moves medially and inferiorly, tilting the glenoid cavity downward. This movement is typical when lowering the arm from an overhead position, bringing it back to the side. The opposite of scapula downward rotation is scapula upward rotation. The levator scapulae contributes to the downward rotation of the scapula.
When acting unilaterally (one side contracts at a time), the levator scapulae muscle can cause lateral flexion and rotation of the neck (specifically ipsilateral rotation) [23]. Lateral flexion refers to the action of tilting the head to the side, towards the shoulder. Rotation involves turning the head to the side.
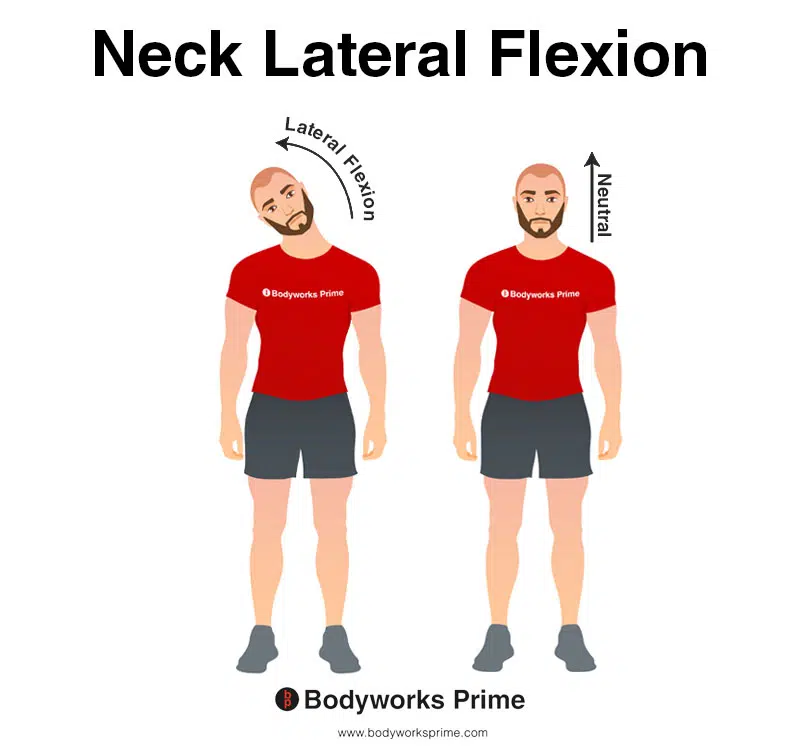
This image demonstrates neck lateral flexion, which involves bending the neck to the side. Unilateral contraction of the levator scapulae muscle can contribute to lateral flexion of the neck.
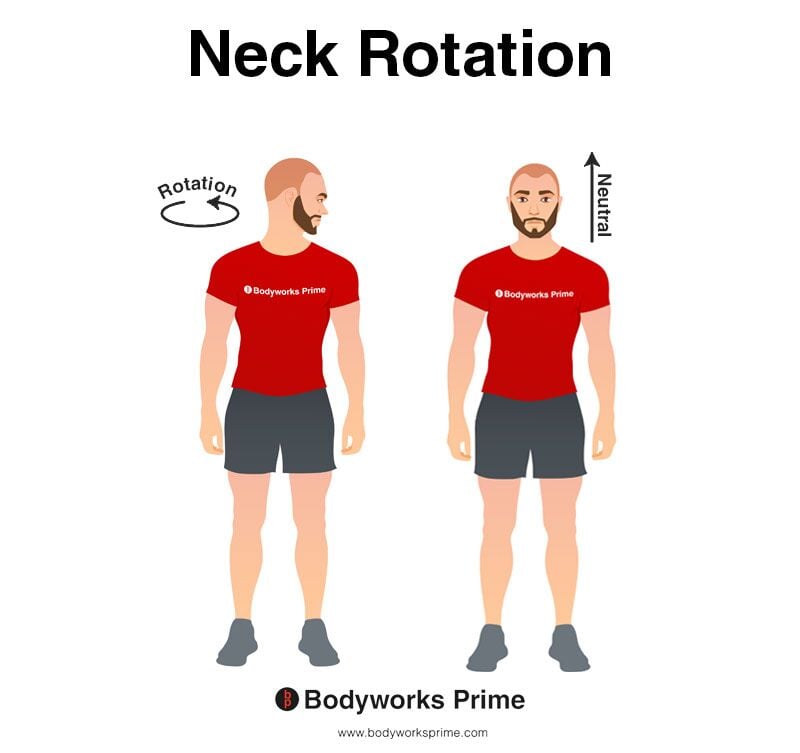
This image demonstrates neck rotation, which involves turning the neck/head to the side. Unilateral contraction of the levator scapulae muscle can contribute to rotation of the neck (specifically ipsilateral rotation).
This muscle also aids in the extension of the neck when both sides contract together (bilateral contraction) [24]. Neck extension is the action of bending the neck backwards, as if looking upward towards the sky.
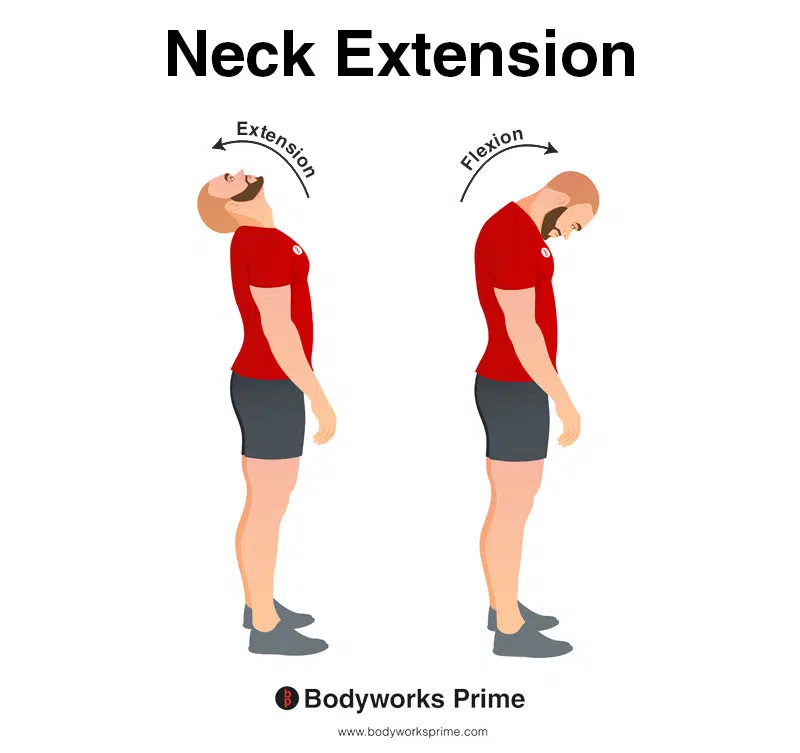
This image demonstrates neck extension, which involves bending the neck backwards. The opposite of neck extension is neck flexion. Bilateral contraction of the levator scapulae muscle can contribute to neck extension.
Innervation
The levator scapulae muscle primarily receives its innervation from the dorsal scapular nerve [25] [26]. The dorsal scapular nerve is a branch of the C5 nerve root, and it emerges from the upper section of the brachial plexus, a complex network of nerves originating from the lower four cervical nerves (C5-C8) and the first thoracic nerve (T1). Being the first nerve branch off the C5 root, the dorsal scapular nerve carries motor signals to the levator scapulae and the rhomboid muscles [27] [28].
In its journey from the nerve roots, the dorsal scapular nerve descends obliquely across the neck towards the posterior surface of the levator scapulae and the rhomboids. It penetrates these muscles and provides them with motor fibers required for their various actions [29] [30].
Aside from the dorsal scapular nerve, the levator scapulae muscle can also receive innervation from the cervical plexus via C3 and C4 cervical nerves [31] [32]. The cervical plexus is a network of nerves formed by the anterior rami (divisions) of the first four cervical spinal nerves (C1-C4). These nerves provide additional innervation and contribute to the complex coordination of muscular actions in the neck and shoulder region [33] [34].
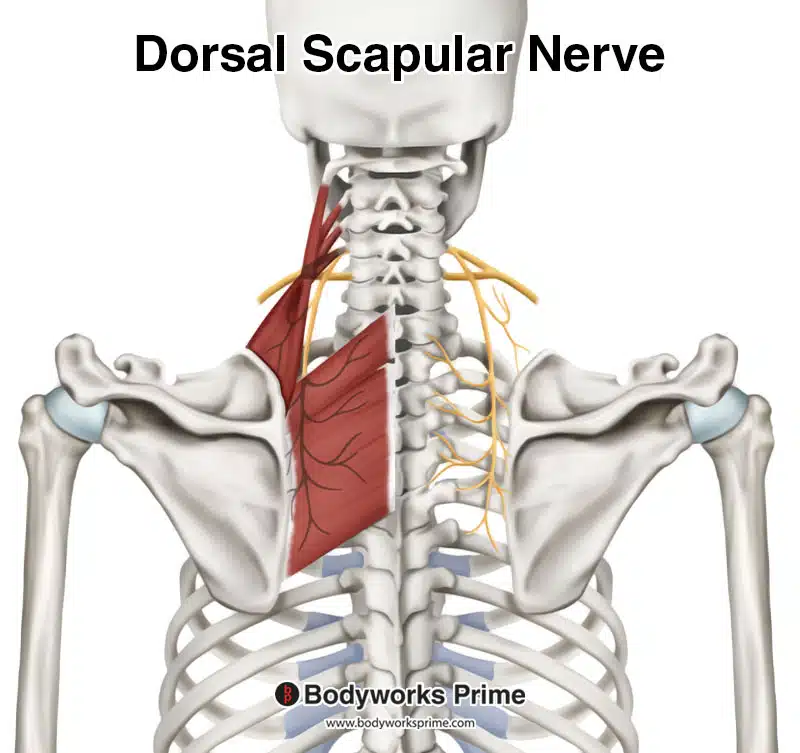
In this image we can see the dorsal scapular nerve which innervates the levator scapulae muscle.
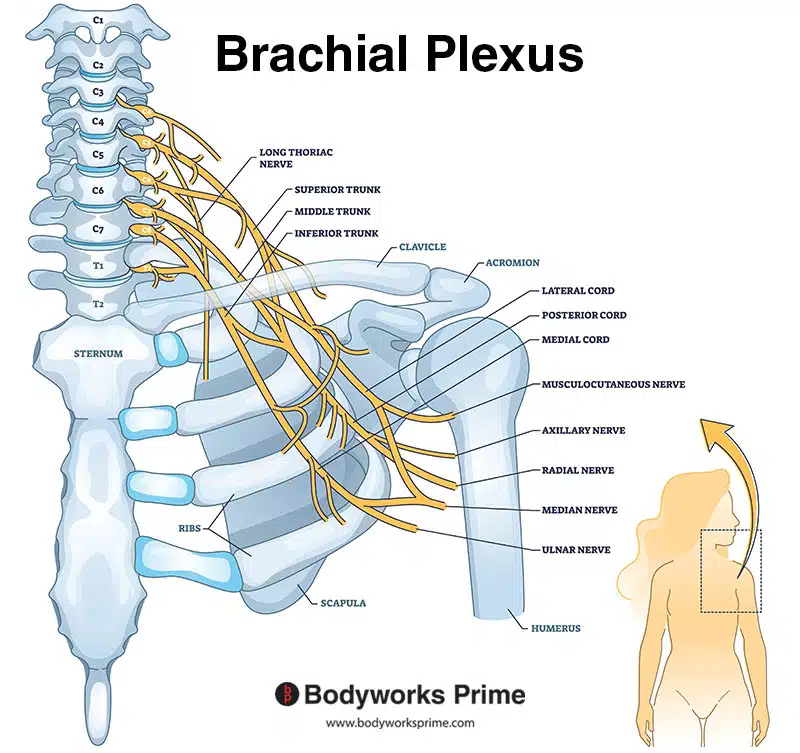
In this image we can see the brachial plexus. The dorsal scapular nerve is a branch of the brachial plexus. The dorsal scapular nerve arises from the brachial plexus, usually from the plexus root of cervical nerve C5. The root is the part of the nerve that is located right next to the vertebra.
Blood Supply
The levator scapulae muscle is predominantly supplied with blood by the dorsal scapular artery. The point of origin of this artery is a topic of discussion in anatomical literature, with the most frequently cited sources being the subclavian artery, or as a branch of the thyrocervical trunk [35] [36]. The thyrocervical trunk is a short artery that originates from the subclavian artery, and its role is to supply blood to multiple structures in the neck and upper back region [37] [38].
The transverse cervical artery, another branch of the thyrocervical trunk, divides into the superior and deep branches at the level of the levator scapulae. The deep branch of the transverse cervical artery is also recognised as the dorsal scapular artery. This artery descends along the medial border of the scapula, providing blood to the levator scapulae and adjacent muscles [39] [40] [41].
Want some flashcards to help you remember this information? Then click the link below:
Levator Scapulae Flashcards
Support Bodyworks Prime
Running a website and YouTube channel can be expensive. Your donation helps support the creation of more content for my website and YouTube channel. All donation proceeds go towards covering expenses only. Every contribution, big or small, makes a difference!
References
| ↑1, ↑4, ↑5, ↑6, ↑19, ↑36, ↑39 | Henry JP, Munakomi S. Anatomy, Head and Neck, Levator Scapulae Muscles. [Updated 2022 Aug 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553120/ |
|---|---|
| ↑2, ↑11, ↑17, ↑27, ↑29, ↑33, ↑37, ↑40 | Standring S. (2015). Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 41st Edn. Amsterdam: Elsevier. |
| ↑3, ↑12, ↑18, ↑28, ↑30, ↑34, ↑38, ↑41 | Moore KL, Agur AMR, Dalley AF. Clinically Oriented Anatomy. 8th ed. Philadelphia: Lippincot Williams & Wilkins; 2017. |
| ↑7, ↑13 | Anderson WS, Lawson HC, Belzberg AJ, Lenz FA. Selective denervation of the levator scapulae muscle: an amendment to the Bertrand procedure for the treatment of spasmodic torticollis. J Neurosurg. 2008 Apr;108(4):757-63. |
| ↑8, ↑14 | Mitchell B, Imonugo O, Tripp JE. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 10, 2020. Anatomy, Back, Extrinsic Muscles. |
| ↑9, ↑15 | Oladipo GS, Aigbogun EO, Akani GL. Angle at the Medial Border: The Spinovertebra Angle and Its Significance. Anat Res Int. 2015;2015:986029. |
| ↑10, ↑16 | Vetter M, Charran O, Yilmaz E, Edwards B, Muhleman MA, Oskouian RJ, Tubbs RS, Loukas M. Winged Scapula: A Comprehensive Review of Surgical Treatment. Cureus. 2017 Dec 07;9(12):e1923. |
| ↑20, ↑22, ↑25, ↑31 | Cowan PT, Mudreac A, Varacallo M. Anatomy, Back, Scapula. 2021 Aug 11. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID: 30285370. |
| ↑21 | Frank RM, Ramirez J, Chalmers PN, McCormick FM, Romeo AA. Scapulothoracic anatomy and snapping scapula syndrome. Anat Res Int. 2013;2013:635628. doi: 10.1155/2013/635628. Epub 2013 Nov 28. PMID: 24369502; PMCID: PMC3863500. |
| ↑23, ↑24 | Eliot DJ. Electromyography of levator scapulae: new findings allow tests of a head stabilization model. J Manipulative Physiol Ther. 1996 Jan;19(1):19-25. |
| ↑26, ↑32 | Muir B. Dorsal scapular nerve neuropathy: a narrative review of the literature. J Can Chiropr Assoc. 2017 Aug;61(2):128-144. PMID: 28928496; PMCID: PMC5596970. |
| ↑35 | Verenna AA, Alexandru D, Karimi A, Brown JM, Bove GM, Daly FJ, Pastore AM, Pearson HE, Barbe MF. Dorsal Scapular Artery Variations and Relationship to the Brachial Plexus, and a Related Thoracic Outlet Syndrome Case. J Brachial Plex Peripher Nerve Inj. 2016;11(1):e21-e28. |










