| Origin | Humeral head: Medial supracondylar ridge of the humerus Ulnar head: Coronoid process of the ulna |
| Insertion | Lateral mid-shaft of the radius |
| Action | Pronation of forearm Contributes to flexion of the forearm at the elbow |
| Nerve | Median nerve (C6-C7) |
| Artery | Branches of the bachial, radial and ulnar arteries |
Location & Overview
The pronator teres muscle is a forearm muscle with both radial and ulnar heads. It is located laterally in the most superficial layer of the anterior muscles of the forearm. The distal anterior surface of the pronator teres is covered by the brachioradialis muscle [1] [2]. The pronator teres muscle gets its name due to is shape and action. ‘Pronator’ refers to its action of pronation and ‘teres’ refers to its shape being long and rounded [3]. Images of the pronator teres are included further down the page.
The median nerve typically passes through the humeral and ulnar heads of the pronator teres muscle. Compression of the median nerve is referred to as ‘pronator teres syndrome.’ However, variations in this arrangement exist, such as the median nerve passing through the muscle belly of the ulnar head of the pronator teres or being situated posteriorly to both muscle heads. In some individuals, the ulnar head of the pronator teres muscle is entirely absent (around 14% of people, according to research by Caetano et al. [2017]) , while in others, the ulnar head is underdeveloped, with only a fibrous band originating from the ulna’s coronoid process (present in approximately 17% of individuals studied by Caetano et al. [2017]) [4]. Although the absence of the ulnar head is rare, when it is missing, the likelihood of median nerve entrapment may be reduced [5].
Irritation of the median nerve due to pronator teres syndrome can result from repetitive or rapid grasping and pronation movements. Activities such as tennis, hammering, rowing, and excessive exercise volume involving these movements by bodybuilders can contribute to median nerve entrapment and pronator teres syndrome. However, pronator teres syndrome is relatively rare, which may sometimes lead to misdiagnosis or confusion with more common conditions, such as carpal tunnel syndrome [6].
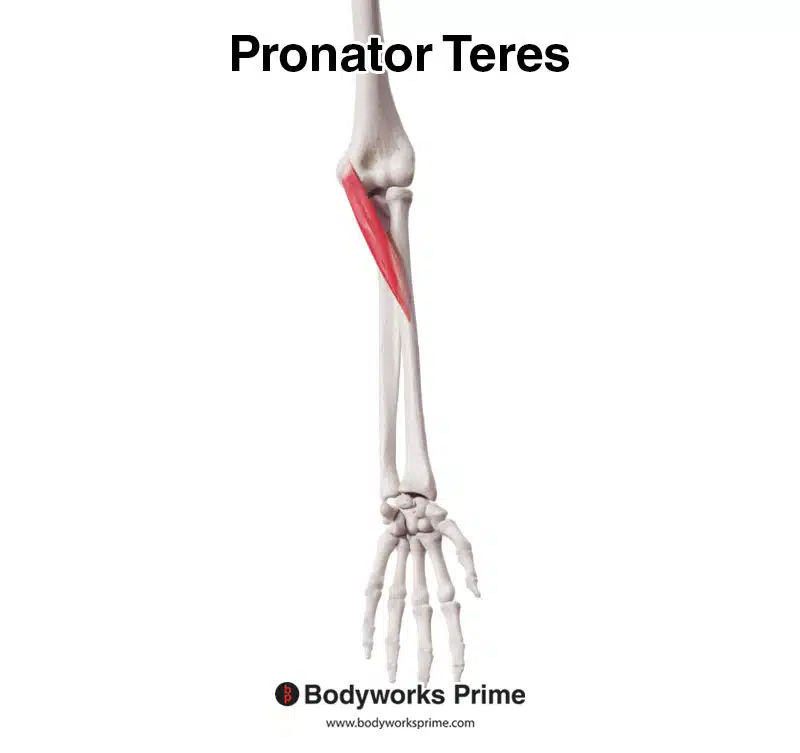
Here we can see the pronator teres from an anterior view.
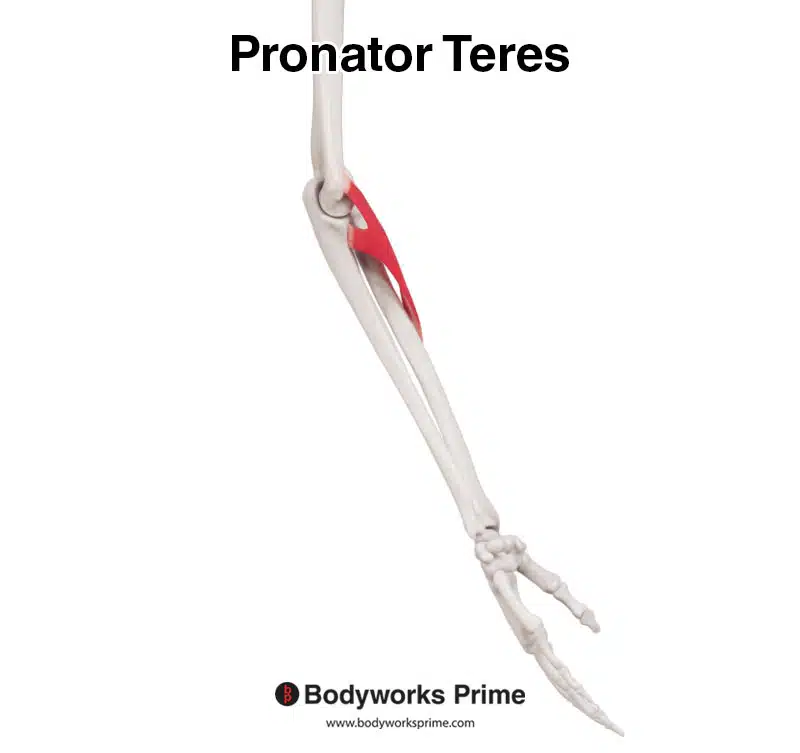
Here we can see the pronator teres from a medial view. This allows us to see the two heads of origin: the larger humeral head and the smaller ulnar head.
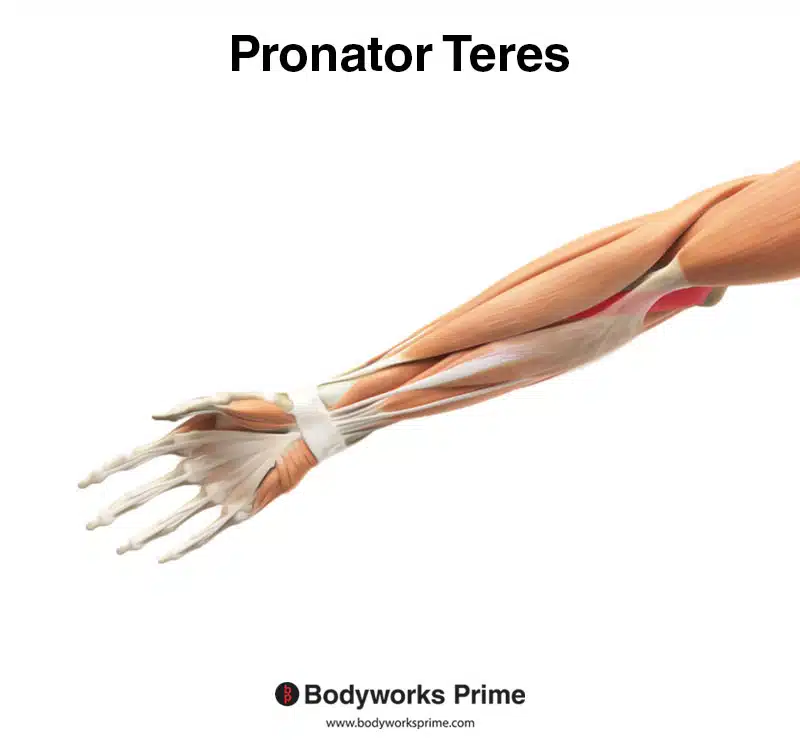
Here we can see the pronator teres highlighted in red, from an anterior view, amongst the other muscles of the arm. You can see the brachioradialis muscle covers the distal part of the pronator teres.
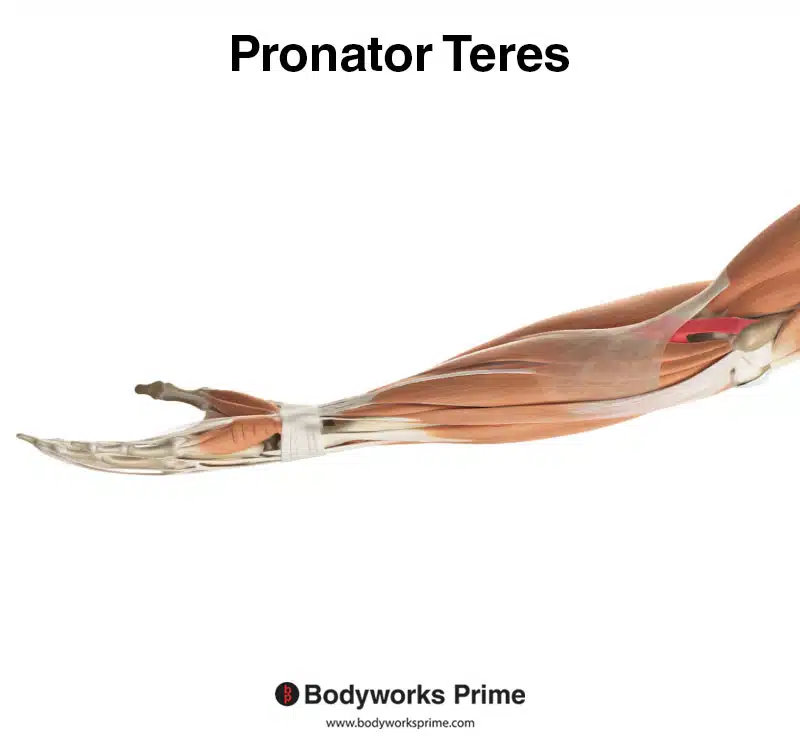
Here we can see the pronator teres highlighted in red, from a medial view, amongst the other muscles of the arm. You can see the brachioradialis muscle covering up the distal part of the pronator teres.
Origin & Insertion
The humeral head, the larger of the two heads, originates from the superior part of the medial epicondyle on the humerus’ medial supracondylar ridge. The smaller ulnar head originates from the coronoid process of the ulna. As the two heads travel down the forearm, they converge to form a common flexor tendon. This tendon then inserts into the middle of the radius’ shaft [7] [8] [9].
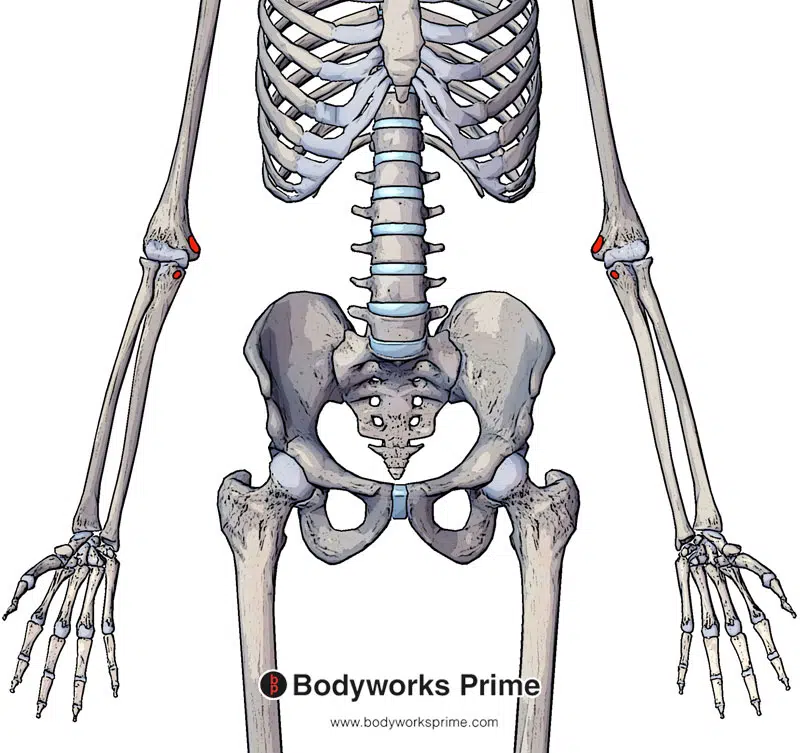
Highlighted in red we can see the origin of the pronator teres muscle. The humeral head’s origin is on the medial supracondylar ridge of the humerus. Whereas the ulnar head originates on the coronoid process of the ulna.
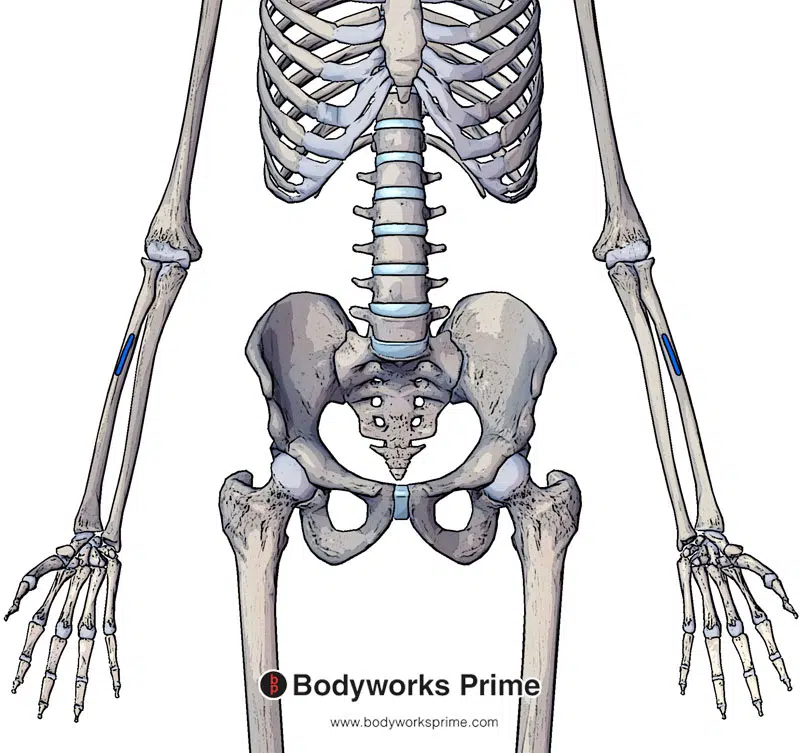
Highlighted in blue we can see the insertion of the pronator teres on the lateral mid-shaft of the radius.
Actions
The pronator teres can perform pronation of the forearm as its main action. It is also able to assist other muscles with performing flexion of the forearm at the elbow joint [10] [11] [12].
These actions are beneficial in sports such as tennis, where forearm rotation is required for various strokes, like backhands and forehands. In baseball, the pronator teres aids in rotating the forearm during throwing and swinging the bat. Additionally, it contributes to forearm rotation during a golf swing. In everyday life, the pronator teres is useful for activities like turning a doorknob or opening a jar, as it helps rotate the forearm to twist the doorknob or lid.
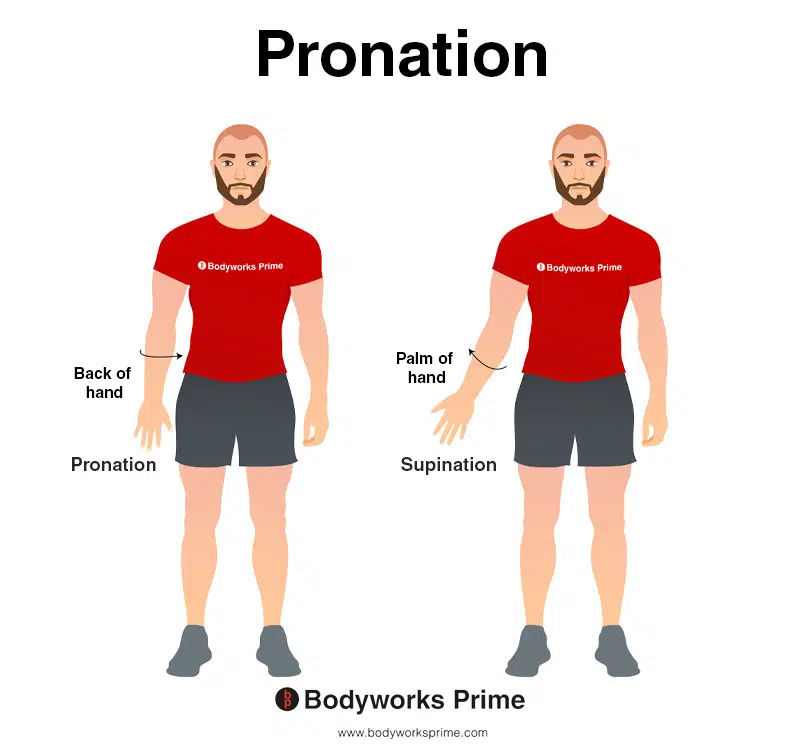
This image demonstrates pronation, where the hand and forearm is rotated so that the back of the hand faces the front of the body, while in the anatomical position. The opposite of pronation is supination. Pronation is the primary action of the pronator teres muscle.
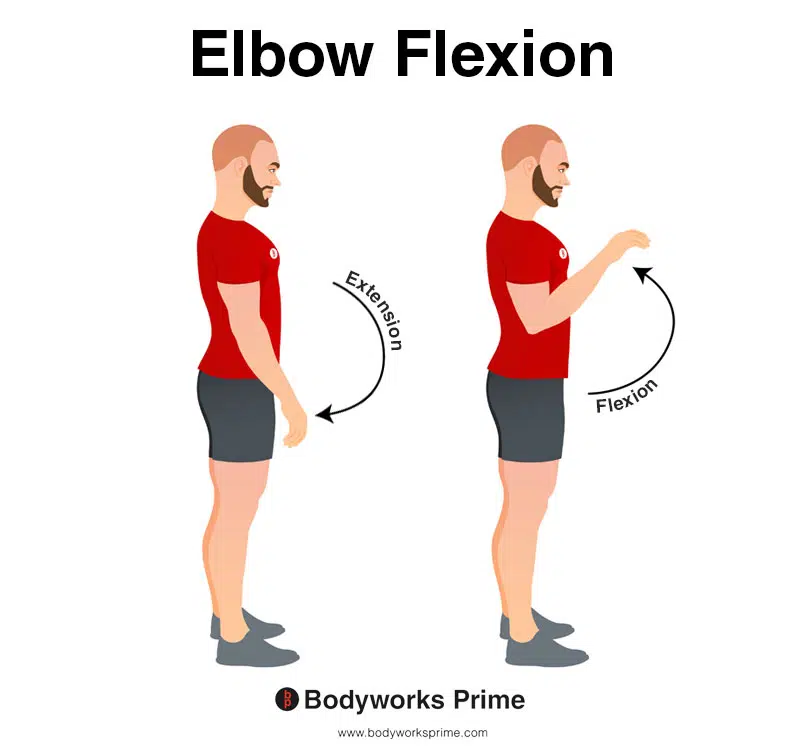
This image demonstrates elbow flexion, which involves bending elbow. The opposite movement of elbow flexion is elbow extension. Assisting other muscles with elbow flexion is a secondary action of the pronator teres.
Innervation
The median nerve innervates both heads of the pronator teres muscle from C6 to C7 roots. The median nerve is a part of the brachial plexus [13] [14].
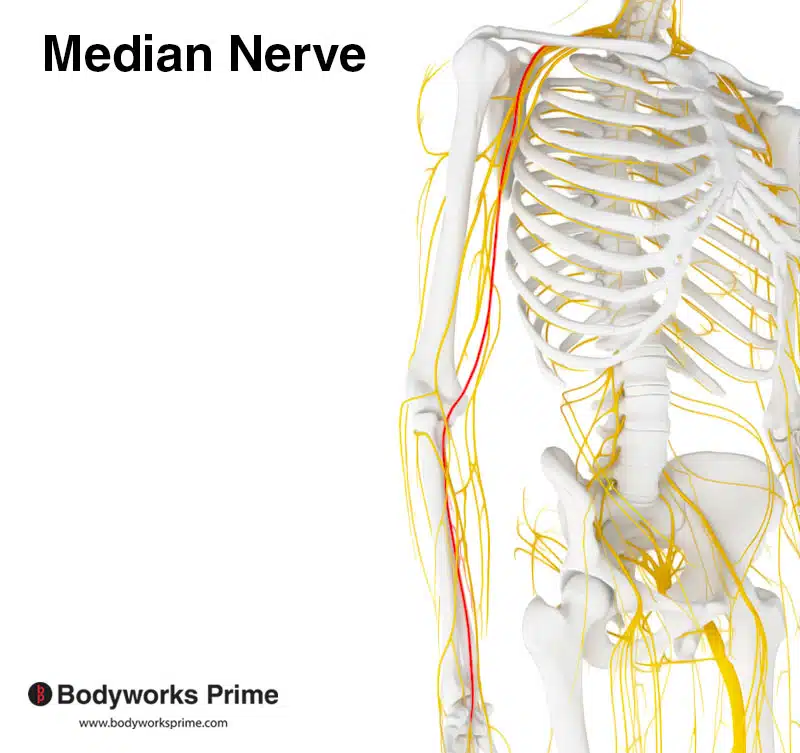
Pictured here we can see the median nerve which innervates the pronator teres. The specific nerve roots which innervate the pronator teres are C6 and C7.
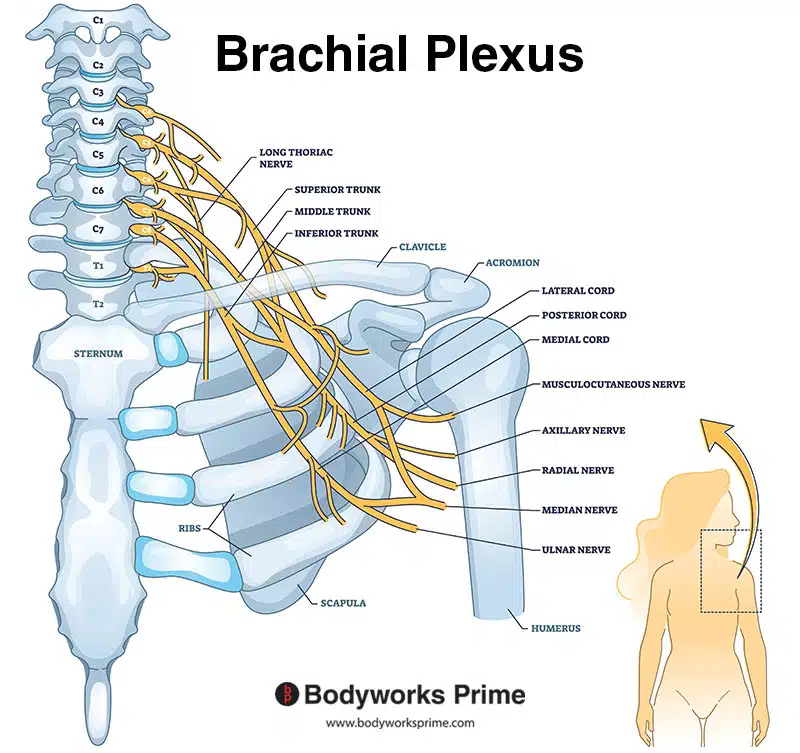
Pictured here we can see the brachial plexus. As you can see from the image, the median nerve is a branch of the brachial plexus.
Blood Supply
Blood is supplied to the pronator teres muscle via the brachial, radial and ulnar arteries [15] [16].
Want some flashcards to help you remember this information? Then click the link below:
Pronator Teres Flashcards
Support Bodyworks Prime
Running a website and YouTube channel can be expensive. Your donation helps support the creation of more content for my website and YouTube channel. All donation proceeds go towards covering expenses only. Every contribution, big or small, makes a difference!
References
| ↑1, ↑12, ↑14, ↑16 | Olewnik Ł, Podgórski M, Polguj M, Wysiadecki G, Topol M. Anatomical variations of the pronator teres muscle in a Central European population and its clinical significance. Anat Sci Int. 2018;93(2):299-306. doi:10.1007/s12565-017-0413-y |
|---|---|
| ↑2, ↑9 | Moore KL, Agur AMR, Dalley AF. Clinically Oriented Anatomy. 8th ed. Philadelphia: Lippincot Williams & Wilkins; 2017. |
| ↑3, ↑5, ↑6, ↑7, ↑10, ↑13 | Dididze M, Tafti D, Sherman Al. Pronator Teres Syndrome. [Updated 2022 Jan 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526090/ |
| ↑4, ↑8 | Caetano EB, Vieira LÂ, Sprovieri FA, Petta GC, Nakasone MT, Serafim BL. Anatomical variations of pronator teres muscle: predispositional role for nerve entrapment. Rev Bras Ortop. 2017;52(2):169-175. Published 2017 Mar 2. doi:10.1016/j.rboe.2017.02.003 |
| ↑11 | Van Hoecke J, Pérot C, Goubel F. Contribution des muscles biceps brachii et pronator teres á l’effort de prono-supination. I. Travail statique (Contribution of the biceps brachii and pronator teres muscles to the efforts of pronation or supination. I. Statistical work (author’s transl)). Eur J Appl Physiol Occup Physiol. 1978 Mar 20;38(2):83-91. French. doi: 10.1007/BF00421525. PMID: 639790. |
| ↑15 | Vymazalová K, Vargová L, Joukal M. Variability of the pronator teres muscle and its clinical significance. Rom J Morphol Embryol. 2015;56(3):1127-35. PMID: 26662149. |










